The USC Tina and Rick Caruso Department of Otolaryngology–Head and Neck Surgery offers comprehensive services for head and neck tumor resection. In each case, our goal is to provide the patient with the best treatment available that has the least impact on functional status.
We offer services including transoral robotic surgery, reconstructive surgery using microvascular free flaps and endoscopic transnasal tumor resection. Our surgeons are also highly skilled in open surgical techniques and will offer these approaches to patients who are not eligible for minimally invasive surgery.
The team of clinicians helping patients manage head and neck cancer includes otolaryngologists, radiation oncologists, medical oncologists and radiologists. As needed, we also incorporate the expertise of other specialists, including plastic surgeons, physiotherapists and speech therapists, to provide patients with the best possible outcomes. The team meets weekly to discuss cases and determine the best treatment approach for each patient.
At Keck Medicine of USC, patients also have access to an array of clinical trials, which may offer therapeutic options that are not widely available. For example, investigators at Keck Medicine of USC are participating in the INSPIRE trial, which offers patients with stage II-IV oral cavity cancer immunotherapy prior to surgery, with the goal of activating the patient’s immune response to improve disease control. The team also started immunotherapy for recurrent head and neck cancer using PD-1 inhibitors and EphB4 peptide, a drug that was discovered and went through clinical trial at the USC Norris Cancer Center. This combination drug therapy has the potential to help patients with incurable cancer who would, otherwise, be placed on hospice care only.
In 2010, the USC Tina and Rick Caruso Department of Otolaryngology–Head and Neck Surgery became the first center on the West Coast to offer transoral robotic surgery (TORS) to treat head and neck cancers. TORS is primarily used to treat cancers of the tonsil and tongue base, most of which are squamous cell carcinoma. These tumors are typically caused by the human papilloma virus and are smaller and less aggressive than oropharyngeal squamous cell carcinoma that is related to tobacco use. Approximately 75 percent of patients with this type of cancer are eligible for TORS, as their tumors are an appropriate size for transoral resection.

Figure 1: Intraoperative picture of TORS dissecting cancer of the left tonsil. (a) Single port robot is gradually deploying its camera and arms in preparation to dissect tumor in the pharynx. (b)
The TORS system employs numerous technological functions, including 3D visualization, a magnified view of the operative field, tremor reduction and motion scaling, that allow our surgeons to successfully remove many tumors. The tip of the surgical instruments can rotate 180 degrees and an angled telescope can tilt up or down 30 degrees. The combination of these articulations gives the surgeon the ability to visualize and access tissue that is otherwise difficult using hand-held or straight instruments.
Most patients undergoing TORS do not need reconstructive surgery following the tumor resection. A TORS procedure can also be combined with external neck dissection of lymph nodes to determine the tumor stage and decide on any further treatment that is necessary. For patients who aren’t eligible for TORS, surgeons can still perform open surgery to resect the tumor. In the near future, investigators will begin enrolling patients in a clinical trial of transoral robotic surgery for oropharyngeal cancer.
The next-generation robot (Intuitive Surgical da Vinci® Sp Single Port Robotic Surgical System) has more flexibility for TORS. The camera and surgical arms are housed in a single port. This new surgical system has the potential to dissect tumors from “hard-to-reach areas” in the head and neck region.
Some patients with head and neck cancers who undergo open resection may need reconstructive surgery following tumor resection. For these patients, one possible procedure is reconstruction with microvascular free flaps. The goal of microvascular reconstruction is to restore form and function for the patient. Specifically, we aim to restore speech, swallowing and normal facial appearance as best as possible. In this procedure, tissue is removed from either the forearm, the thigh or the fibula to reconstruct the tissue defect of skin, muscle or bone of the head or neck as necessary.
A 65-year-old male was seen at Keck Medicine of USC for a mass on the right side of the neck that the patient found while shaving. The patient completed a course of antibiotics but the mass did not resolve. The patient didn’t report any dysphagia or throat pain and had no history of smoking.
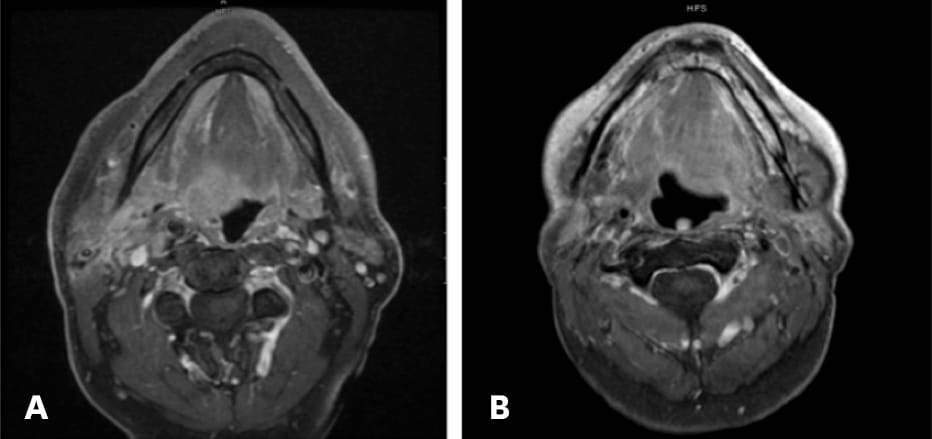
Figure 2: Preoperative axial MR image showing a 2.5 centimeter diameter mass in the right base of the tongue (red arrow) and bilateral abnormal, enlarged lymph nodes. (a) Postoperative MR image shows that the right-side mass was totally removed using TORS. (b)
Upon examination, the otolaryngologist found a firm mass in the base of the tongue and an enlarged lymph node on the right side, which were both confirmed by MR imaging (Figure 2a). An endoscopy confirmed a 2.5 centimeter diameter mass on the right side of the tongue that did not cross the midline and a biopsy indicated that the mass was a squamous cell carcinoma.
The otolaryngologist treated the patient with a partial glossectomy and partial pharyngectomy both using TORS (Figure 2b). In addition, a bilateral neck dissection was performed, and the patient underwent postoperative radiotherapy.
After surgery and radiotherapy, the patient retained normal swallowing function and only occasionally experienced a dry mouth that limited his consumption of certain foods. At six years of follow-up, the patient shows no signs of disease.